Roughly 1 out of 70,000 newborns is born with neonatal Alagille syndrome. This condition is often present at birth, though it can take several years for the symptoms to become present. Here are some important facts that parents need to know about neonatal Alagille syndrome.
What Is Neonatal Alagille Syndrome?
Neonatal Alagille Syndrome is a type of genetic disorder that children can inherit from their parents. People with neonatal Alagille syndrome have a mutated or missing copy of a gene labeled Jagged1 on chromosome 20. Problems with this gene are associated with a wide range of liver, heart, and eye problems. Due to a variety of skeletal abnormalities, people with neonatal Alagille syndrome tend to have a very characteristic appearance. Alagille syndrome is also referred to as Alagille-Watson syndrome, syndromic bile duct paucity, or arteriohepatic dysplasia.
What Are the Neonatal Alagille Syndrome Symptoms?
Not all people with neonatal Alagille syndrome have the same symptoms present. The condition can just cause minor issues like some changes to facial features, or it can cause severe heart and liver disease. Some of the most common symptoms include:
- Deep-set eyes
- Straight nose
- Triangular face shape with pointed chin
- Jaundice
- Heart murmurs
- Cardiac anomaly
- Short height
- Butterfly shaped vertebrae
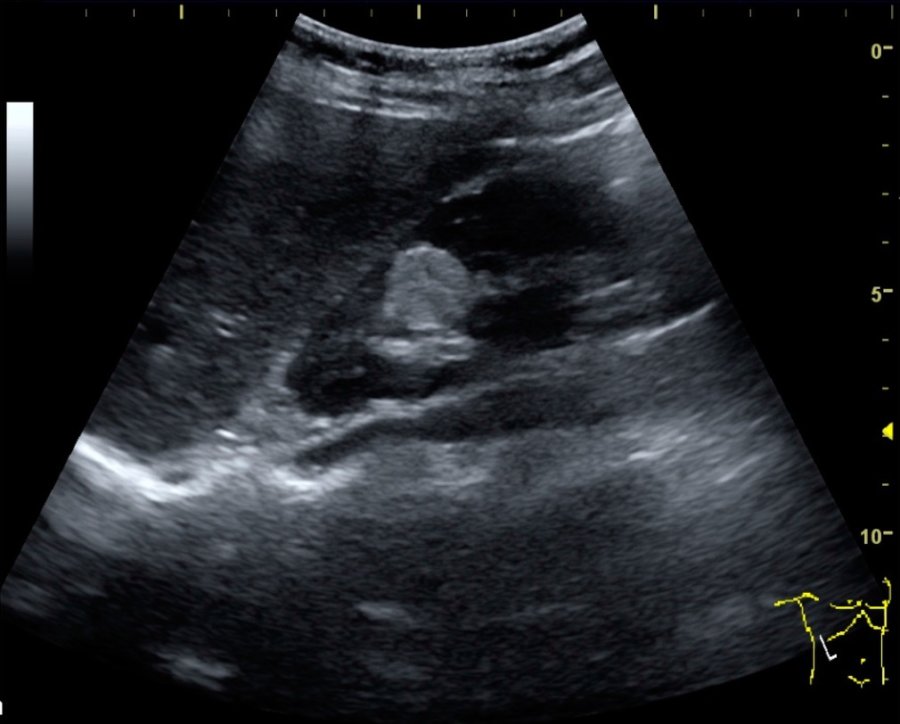
- Kidney abnormalities
- Eye abnormalities
Parents should keep in mind that some symptoms, like kidney abnormalities, can take a while to notice. Signs that these organs are not functioning properly can include chronic itchiness, fatigue, pale skin, fluid retention, weakness, or abnormally pale feces.
How Is Neonatal Alagille Syndrome Treated?
Treatment for neonatal alagille syndrome typically relies on what symptoms the patient is presenting. Many children have mild enough Alagille syndrome that they just need to eat a healthy diet and get plenty of rest to help with issues like delayed puberty or failure to thrive. Certain medications can help with things like improving bile function, stabilizing kidney function, and helping the heart run properly. However, in more serious situations, surgery may be necessary. Surgeries can help to correct skeletal issues, replace malfunctioning kidneys and livers, or treat cardiac abnormalities.